Consultant Cardiac Anaesthetist and Intensivist working in the Wessex Cardiac Unit in University Hospital Southampton. Clinical interests include paediatric cardiac anaesthesia & perioperative echocardiography.
Patients with right to left shunt have decreased pulmonary blood flow and can be intermittently or permanently cyanosed. The classic example is tetralogy of Fallot where a large VSD co-exists with an obstruction to blood flow from the RV to the PAs hence causing right to left shunt or ‘spells’. Like many things this is a spectrum of limited to severe right to left shunt
Theatre B is the home of childrens heart surgery in Southampton. Drs Curry, Wilkinson, Al-Azzawi, Montague, Huber, Wessels & Bakalova all undertake these lists.
Congenital cardiac surgery is a complex and fascinating subspecialty that can sometimes be intimidating to residents and fellows, but we have all the exposure and facilities in Southampton to train people to undertake this endlessly challenging and rewarding discipline.
In the OR most cases have some emergency medications drawn up. As most of our patients are babies we do not index emergency meds by weight but rather use a ‘one size fits all’ approach. For any sick cardiac baby the following is appropriate: 1ml of atropine (blue needle attached), 1ml of sux (blue needle attached), 5 mls of calcium gluconate, 10 mls of 10 mcg/ml adrenaline (this is made with 1 ml of a minijet 1:10,000 diluted with 9 mls 0.9% NaCl, 10 mls of 1 mcg/ml adrenaline (this is made by taking one ml of the 10 mcg/ml syringe and diluting it with a further 9 mls of 0.9% NaCl.
Heparin at a slightly augmented dose of 400 IU/kg is prepared (due to lower average levels of antithrombin 3), an ACT syringe and ABG are all prepared in OR as usual.
Most consultants will vary with precise medications used but as a guide:
Fentanyl: 20 mcg/kg
Midazolam: 200 – 400 mcg/kg
Sometimes propofol 2-3 mg/kg
NDMR (such as vecuronium 0.1-0.2mg/kg, pancuronium 0.2mg/kg, or rocuronium 1 mg/kg)
Cefuroxime: 30 mg/kg (2 doses)
Tranexamic acid: 30 mg/kg
If aprotinin is used it is usually for complex multi-redo sternotomies or predicted extremely long CPB runs at a dose of 30,000 U/kg bolus then 30,000 U/kg to the pump then 10,000 U/kg/hr until CPB discontinues.
phenylephrine 100mcg/ml in 10 mls for the perfusionist.
[Phenylephrine is rarely drawn up routinely for paeds cardiac]
Blood products:
Currently all paediatric patients presenting for heart surgery have a “hypo pack” prepared for them. This consists of RBC for transfusion and a bag of appropriate platelets (approx 250 mls) on the rocker. If any blood products are required we call extension 4620 1 hour in advance and request verbally for products to be prepared. If clotting factors are required < 1 year then octaplas is used, if > 1 year FFP or PCC (currently prothromplex) as an alternative/adjunct.
If the patient requires inotropes then the B agonist of choice is dopamine. The preparation schedule is on the cupboard in theatre B. Dopamine 15mg/kg is drawn up from the 40mg/ml ampoule and mixed with 5% dextrose to make 50 mls. 1 ml/hr of this mix = 5 mcg/kg/hr
MIlrinone is a frequently used inotropes in paediatrics and is drawn up as 10mg (=10mls) and diluted with 40 mls of 5% dextrose to make 50 mls. For most babies a dose range of 0.25-0.5 mcg/kg/min is appropriate
If needed our techs can arrange inhaled nitric oxide (iNO) on bleep 2317. They will help connect to the theatre breathing circuit and we usually will start at a dose of 20ppm.
Prior to transferring to PICU at the end of the case the case must be ended on metavision and the patient assigned to the correct clinical area on the check out screen and PICU called on 6972 to make sure everything is ready prior to departure.
In UHS we perform between 300-400 paediatric cardiac cases per year. During your attachment you may well have the opportunity to join the congenital team in theatre B. Dr Andy Curry is the lead for congenital anaesthesia in UHS and the team also consists of a number of other consultant paediatric cardiac anaesthetists: Dr Gareth Charlton, Dr Mike Herbertson, Dr Jonathan Huber, Dr James Montague, Dr Tom Pierce & Dr Kirstin Wilkinson all undertake these lists.
We perform complex congenital surgery with the full back up of the PICU/surgical/perfusionist ECMO team. The majority of these cases have great outcomes and overall the survival in UHS and the UK is excellent. Full details of UHS outcome data is open resource material and found here. It is worth reading to understand the effort & quality being delivered in your home centre. We also undertake some incredibly high risk cases and our communication and professionalism with the parents of these children needs to be of the highest order.
This section mean to explain some of the basic set up of a paediatric cardiac case in UHS so you might understand the stages specific to a baby having heart surgery.
All patients are pre assessed the day before heart surgery. They are brought into E1 ward and the nursing team there are very organised and helpful at getting everything ready for the assessing anaesthetist. We use the normal pink anaesthetic card but note that children won’t necessarily have the same pre-op investigations: PFTs and angiograms are often unnecessary as these assess acquired diseases.
The majority of paediatric cardiac surgery is for babies. Most children have an IV sited by the E1 team allowing for IV induction, sometime an inhalational induction is mandatory however and this should be discussed with the parents. Most consultants are happy for parents to accompany their child to the anaesthetic room however it should be noted that in children < 6m age there is no separation anxiety for the child – it is for the parents benefit. As such, some parents when distressed choose not to come into the AR.
Monitoring is established via ECG and Massimo pulse oximetry, BP can be measured with NIBP. An IV induction is usual. There are many ways to skin a cat but most of us now favour a balanced anaesthetic using moderate doses of fentanyl (2mcg/kg) and midazolam (0.2mg/kg) and a NDMR. Other agents such as propofol and thiopentone clearly work and it mostl
This is a synopsis of HIT as assessed and managed in CICU. It is not all inclusive but aims to promote awareness in clinicians practicing cardiac anaesthesia & CICU.
Please can all trainees and fellows read and familiarise yourself with the resources available on Metavision as described below. In addition there are 2 pdf’s attached which the AAGBI recommend.
HIT:
Higher than usual incidence in cardiac surgery ~ around 1-5% depending on population.
Type 2 HIT is a life threatening condition after exposure to unfractionated heparin (although LMWH carries a 50% cross reactivity)
HIT2 is an immune mediated hypersensitivity reaction caused by IgG antibodies to heparin and platelet factor 4 (PF4)
IgG antibody testing has high false positive rate (up to 60%)
Negative IgG excludes HIT but the results take 4-7 days
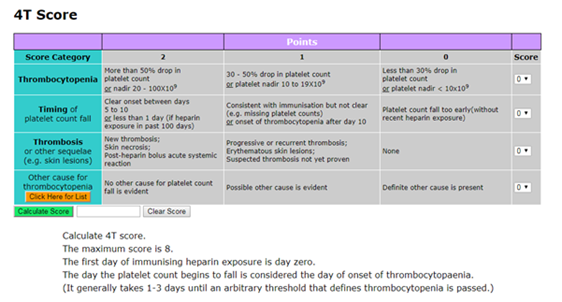
Presentation: Diagnosis is the key (Pdf 1 is a useful resource). This is done using the 4T score which quantifies the degree of thrombocytopenia, the timing of the thrombocytopenia & the degree of thrombosis. This is available in Metavision (location described below):
If HIT is suspected the duty CICU consultant must be notified. A 4T score of 4 or more warrants clinical diagnosis and initiation of investigations and treatment for HIT
Mode of death with HIT is invariably related to systemic thrombosis and treatment is aimed at minimising this risk
Heparin is discontinued immediately, plt count monitored, warfarin must also be avoided or reversed (with vit K) as it can cause extensive skin and organ necrosis in up to 70% patients
Evaluate for presence of DVT (USS/CT)
Plt transfusions are only indicated if there is severe bleeding in the context of severe thrombocytopenia otherwise they ‘feed’ the prothrombotic process
After diagnosis treatment involves systemic anticoagulation
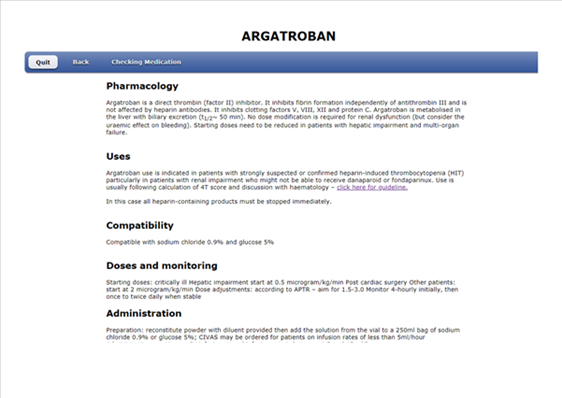
In UHS this is with ARGATROBAN (a direct thrombin inhibitor) by infusion
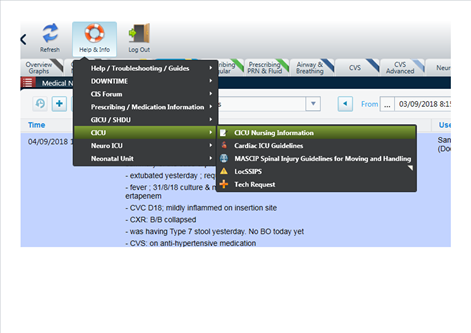
Argatroban is hepatically cleared with t1/2 of 50 mins. It is safe to use in renal failure but if there is hepatic dysfunction a dose reduction is required (usually around 75%). The protocol is available on metavision & accessed via the “Help & Info” tab shown below:
The HIT guideline can be found on MetaVision
This brings up the following screen in your web-browser. A number of pathways / protocols are available including the one for HIT:
Within this guideline there is a review of HIT, a 4T calculator, a flowchart for guidance and a protocol for argatroban use:
Interestingly there have been papers published looking at the use of pre-operative plasma exchange followed by conventional heparin/protamine anticoagulation for cardiac surgery in HIT 2 IgG +ve patients which appears to be a safe strategy (although high numbers of tranplant patients in the data). This topic should hopefully appear on a Friday morning meeting in the future to allow group discussion of practice.
These are a series of free to access articles released by the American Society of Echocardiography which are good CPD for specialists and absolute gold for those training for exams be they EACTA, BSE or the PTExAM: