CAG Rapid Update: Heparin Induced Thrombocytopenia
This is a synopsis of HIT as assessed and managed in CICU. It is not all inclusive but aims to promote awareness in clinicians practicing cardiac anaesthesia & CICU.
Please can all trainees and fellows read and familiarise yourself with the resources available on Metavision as described below. In addition there are 2 pdf’s attached which the AAGBI recommend.
HIT:
Higher than usual incidence in cardiac surgery ~ around 1-5% depending on population.
Type 2 HIT is a life threatening condition after exposure to unfractionated heparin (although LMWH carries a 50% cross reactivity)
HIT2 is an immune mediated hypersensitivity reaction caused by IgG antibodies to heparin and platelet factor 4 (PF4)
IgG antibody testing has high false positive rate (up to 60%)
Negative IgG excludes HIT but the results take 4-7 days
Presentation: Diagnosis is the key (Pdf 1 is a useful resource). This is done using the 4T score which quantifies the degree of thrombocytopenia, the timing of the thrombocytopenia & the degree of thrombosis. This is available in Metavision (location described below):
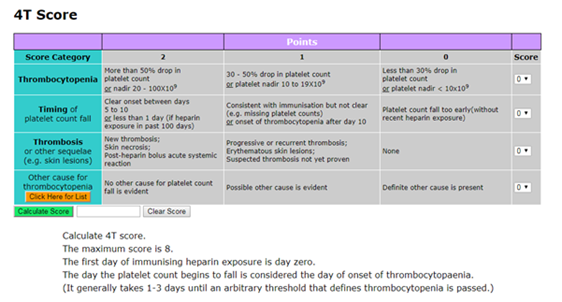
If HIT is suspected the duty CICU consultant must be notified. A 4T score of 4 or more warrants clinical diagnosis and initiation of investigations and treatment for HIT
Mode of death with HIT is invariably related to systemic thrombosis and treatment is aimed at minimising this risk
Heparin is discontinued immediately, plt count monitored, warfarin must also be avoided or reversed (with vit K) as it can cause extensive skin and organ necrosis in up to 70% patients
Evaluate for presence of DVT (USS/CT)
Plt transfusions are only indicated if there is severe bleeding in the context of severe thrombocytopenia otherwise they ‘feed’ the prothrombotic process
After diagnosis treatment involves systemic anticoagulation
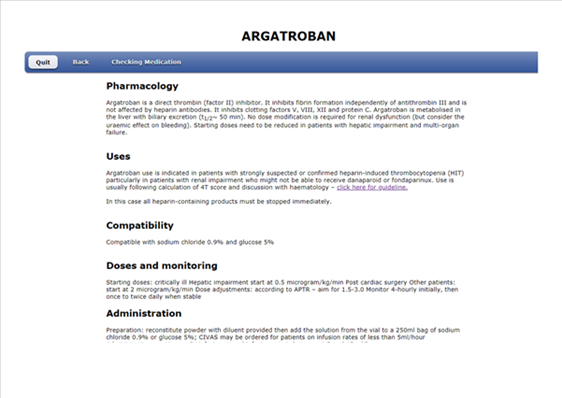
In UHS this is with ARGATROBAN (a direct thrombin inhibitor) by infusion
Argatroban is hepatically cleared with t1/2 of 50 mins. It is safe to use in renal failure but if there is hepatic dysfunction a dose reduction is required (usually around 75%). The protocol is available on metavision & accessed via the “Help & Info” tab shown below:
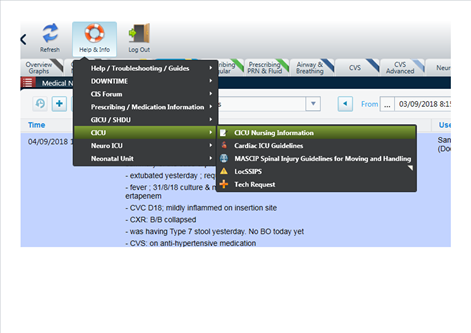
This brings up the following screen in your web-browser. A number of pathways / protocols are available including the one for HIT:

Within this guideline there is a review of HIT, a 4T calculator, a flowchart for guidance and a protocol for argatroban use:
- Interestingly there have been papers published looking at the use of pre-operative plasma exchange followed by conventional heparin/protamine anticoagulation for cardiac surgery in HIT 2 IgG +ve patients which appears to be a safe strategy (although high numbers of tranplant patients in the data). This topic should hopefully appear on a Friday morning meeting in the future to allow group discussion of practice.
Kind Regards,
JPM
